[1] Cochener-Lamard, B. Refractive IOL Patterns are Evolving with the Times. Euro Times Supplement. June 2019. p. 2
[2] PanOptix product information p. 10
Schedule your consultation:
Losing our reading vision has always seemed to me to be one of life’s cruelest jokes. When we are young and can run far we can see up close. When we are old and can’t run far we can’t see up close. Prior to cataract surgery, patients mitigate this problem with progressive glasses that offer distance, intermediate, and near. Interestingly, when patients are offered the choice between a bifocal and a trifocal/progressive glasses in the optical at our practice, 94% choose the more complete visual solution of a trifocal/progressive. This solution seems old fashioned to them and not elegant, but functional.
When it comes to modern cataract surgery with femtosecond lasers and “advanced technology lenses” patients anticipate trifocal vision as the bare minimum we have already trained them to expect. In the past, all we had were bifocal intraocular lens (IOL) options. When we told patients we could only offer a bifocal solution, they stared at us incredulously like we were backwards cavemen. They were expecting something more elegant, not less.

Some patients have bifocal lifestyles so they find this option completely acceptable. For example, an individual that spends 10 hours per day on the computer and reads electronic books rather than paper books mostly needs distance and intermediate vision so a far/intermediate bifocal IOL would work great for them. Others mostly read paper books with very little computer time so a far/reading bifocal lens would work great for them. Many patients, however, spend equal time with computer and paper books and would prefer a trifocal IOL option that would give far, intermediate vision, and close-up reading.
Outside the United states there are multiple trifocal IOL options available like the AT-Lisa, Fine Vision, and the PanOptix. What happens when trifocal IOL lenses are introduced into the standard mix of bifocal/EDOF lenses that we currently have? The simple answer is that the trifocal lenses have tended to quickly become a preferred choice for a significant part of the market. For example, in a 2017 survey done by the ESCRS for its members, respondents indicated that 45.2% of their patients that received a presbyopia correcting lens (lenses that correct for more than just far vision) received a trifocal IOL.1 In Canada, that number is understood to be even higher. The first trifocal IOL to be approved in the U.S. is the PanOptix where it has quickly dominated the advanced technology market.
The bifocal multi-focus and EDOF lenses split the available light into two focal points, one for distance and one for either near or intermediate. The trifocal multiple-focus lenses splits the light into three focal points, distance, intermediate, and near.
The AT-Lisa lens and the Fine Vision lenses (only available in Europe) use a sequential diffractive pattern to achieve their trifocality. This means that the near vision distance, mathematically, will always be exactly half the intermediate distance. These lenses therefore have intermediate at approximately 80 cm (31.5 Inches) and near at approximately 40 cm (15.75 Inches).
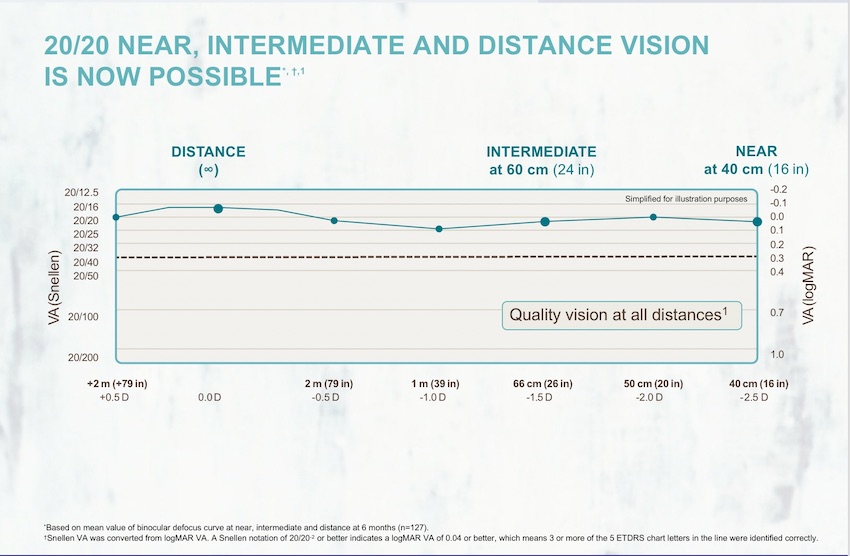
The PanOptix is the most popular trifocal lens in Europe and Canada, and is the only trifocal IOL available in the U.S. The PanOptix engineers started with the goal of providing near vision at 40 cm but wanted an intermediate distance of 60 cm (23.62 inches) based on data they had about patients’ preferences. To achieve this, they started with a quadra-focus design which would have had distance, 120 cm, 60 cm, and 40 cm focal points, but they directed all of the light from the 120 cm peak back to distance. This created a trifocal lens with distance, 60 cm, and 40 cm defocus peaks. This also makes the PanOptix a distance dominant lens by directing a greater amount of the light to enhance distance vision.

Defocus curves are used to help evaluate where patients can see well with a given lens. The data from the FDA trial is presented in the following graph which shows the quality of vision (VA) on the Y axis. This data has been converted to a standard Snellen scale to make it easier to understand. In the Snellen scale, 20/20 vision is considered outstanding. 20/16 vision is even better than 20/20. 20/40 vision (the dotted line) is worse than 20/20 vision and is the minimum requirement for an unrestricted drivers license. The X axis basically shows where the vision was evaluated. For example, how well could patients on average see at distance, intermediate (24 inches) or near (16 inches)
The PanOptix Lens has far intermediate and near vision in focus for most patients. A monofocal lens is a basic IOL that only has one distance in focus. Most patients choose to have far vision in focus, so these monofocal IOL patients need to wear glasses for intermediate vision and near vision.
As each new IOL comes to the U.S. we will be able to study the patient questionnaires from their various FDA studies to try to quantify these quirks. Interestingly, 99.2% of the patients in the PanOptix FDA trial indicated they would have the same lens implanted again.(See the table below)[2] To my knowledge this is the highest rate of satisfaction we have ever seen for a multivocus/EDOF lens! However, it is important to note that it also means that about 1 out of every hundred patients would not have the same lens implanted.
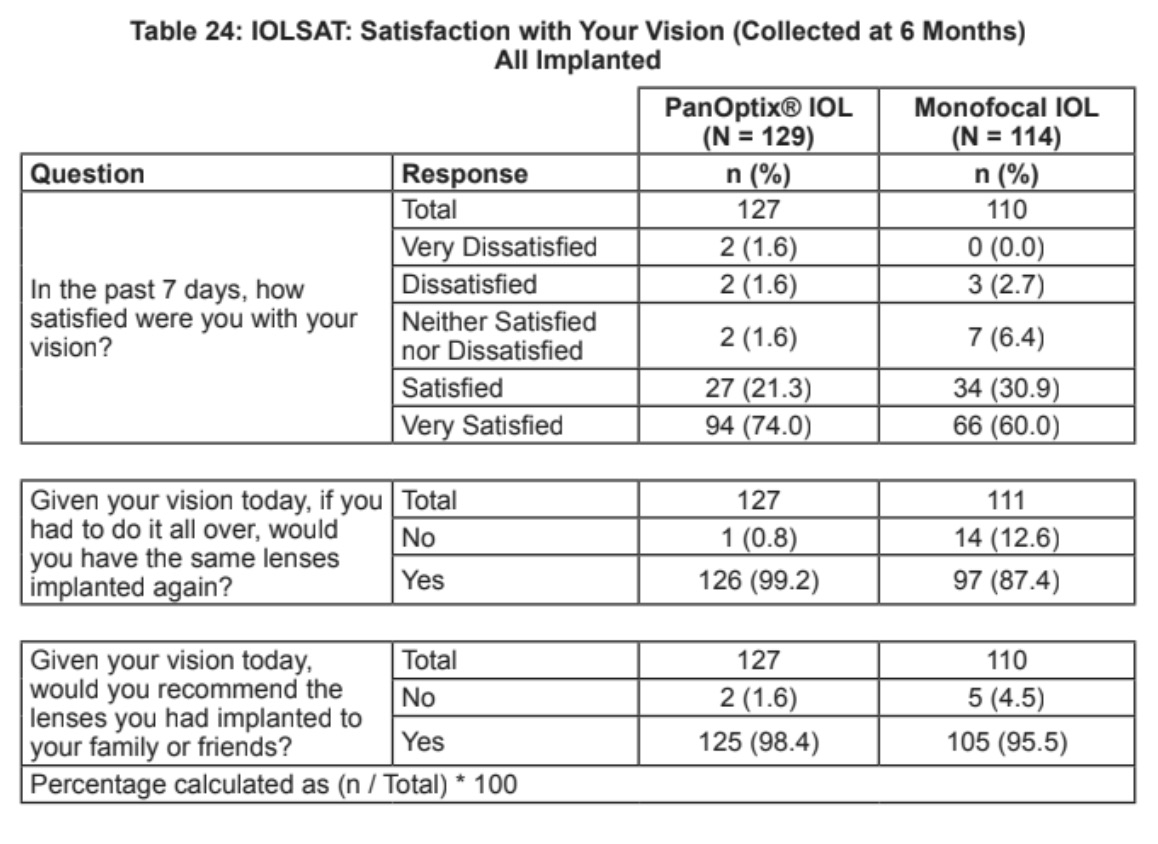
It is equally noteworthy that 95.3% of PanOptix pateints were either satisfied or very satisfied with their vison compared to 90.9% with the monofocal IOL. In addition, 3.2% of PanOptix patients were either very dissatisfied or dissatisfied compared to 2.7% with the monofocal IOL patients.
The bottom line is that patients have cataract surgery because they are not satisfied with their natural lenses that have turned into cataracts and made their vision cloudy. We compare that dissatisfaction with the fact that no man made lens is going to be perfect, but most are profoundly better than the cataract lens that patients are having removed.
No, multiple focus lenses are right for some patients and not for others. For one thing, they cost more than monofocal lenses and patients, not their insurance, bear that extra expense. Money is, by far, the main reason patients may choose to not have an advanced technology lens implanted.
In addition, multiple focus (including EDOF) lenses split light. That is how they allow you to see both near and far at the same time. This also means that each image has less light intensity. Presenting lesser amounts of light in images can affect the quality and contrast of the images. Most patient can’t detect these subtle changes, but some can. The trifocal lenses are still multiple focus lenses and bring with them the attendant quirks that are the lot of all light-splitting IOLs. Among the various multiple focus/EDOF lenses, there are some that have more or less of these quirks, but they all have them.
Night halos can occur with any IOL. Fortunately, these are usually profoundly less than the night glare that the cataracts cause so patients experience an upgrade in night vision by having their cataracts removed. Night halos are more common with multiple focus lenses than with monofocal lenses. As a result, some well-informed patients will continue to prefer monofocal lenses and others will prefer multiple focus lenses. To put the concerns of money, light splitting, and night haloing into perspective, consider a deeper review of the patient satisfaction data above.
The trifocal multiple focus lenses offer a new set of features that line up more closely with the desires of a large percentage of my patients compared to other multiple focus/EDOF options, but their light splitting strategy does not necessarily play to the needs of every patient. For example, short armed-individuals that read four hours per day and do intricate crafting may see better with a stronger, closer reading point like the ZMBOO. An individual with a bifocal lifestyle like a computer programmer may prefer a Vivity Lens to direct most of the near light to an intermediate target. The Vivity Lens appears to have much less night haloing than the PanOptix Lens. In addition, patients with previous refractive surgery or aberrated corneas may achieve higher quality vision with the small pupil optics of an IC 8 lens (not a multiple focus lens and not FDA approved yet at the time of this writing).
Prior to the FDA approval of the PanOptix Lens, this was my percentage of use with the various presbyopia lenses:
58% Symphony
35% ReSTOR 3.0
6% ReSTOR 2.5
1% ZMBOO
74% PanOptix (Patients with a trifocal lifestyle OK with some night haloing)
25% Vivity (Patients with a bifocal lifestyle that prioritize less night haloing)
1% Symphony, ReSTOR, ZMBOO
I was in the FDA trial for the IC8 lens which I would begin implanting in those that have aberrated corneas and those with previous RK if approved.
Start by asking your optometrist which ophthalmologist (eye surgeon) in your region has the best results and has the most experience with advanced technology IOLs like the Panoptix IOL. Often, these types of surgeons also do laser cataract surgery rather than just doing all of their surgeries by hand. Ask your friends who they would recommend as an ideal eye surgeon. You may be surprised to find that many of them have already had cataract surgery! Then meet with your eye surgeon, describe your lifestyle and your desires for your vision for the rest of your life, and ask which IOL would best fulfill your aspirations.
Gary Foster, MD is a Colorado/Wyoming based cataract and refractive surgeon. If you desire any further help, please contact us for a consultation.